
Peptides are one of the most talked-about tools in performance and health optimization right now, but understanding peptide administration is where most people hit a wall. The assumption that you can just swallow a capsule and get the same results as an injection is widespread and wrong. Digestion breaks peptides apart before they reach your bloodstream, which means route of administration isn't a minor detail — it's the difference between a protocol that works and one that doesn't. This guide walks you through the science, the preparation steps, the safety realities, and the smart practices that separate informed users from the ones flying blind.
Table of Contents
- Why injectable peptides are the primary administration method
- Current evidence and clinical uncertainties in peptide dosing and administration
- How to prepare and safely administer peptide injections: Essential steps
- The importance of product quality and sterility in peptide administration
- Best practices for optimizing personalized peptide administration
- A fresh take on peptide administration: navigating uncertainty with informed caution
- Explore personalized peptide therapy support with Peptide AI
- Frequently asked questions
Why injectable peptides are the primary administration method
If you've ever wondered why peptide therapy basics always seem to circle back to needles, the answer is bioavailability. Therapeutic peptides have very low oral bioavailability of around 1 to 2% due to enzymatic degradation in the digestive tract and the physical barrier posed by molecular size. Swallowing a peptide is, in most cases, a waste of it.
Peptide molecules are simply too large and too fragile to survive the digestive gauntlet. Stomach acid and enzymes like proteases break them down into amino acid fragments that no longer carry the signaling function you're after. The gut wall adds another barrier, as most peptides lack the specific transport mechanisms needed to cross intestinal epithelium intact.
Subcutaneous peptide use sidesteps all of this. Injecting into the fatty tissue just beneath the skin delivers the compound directly into the systemic circulation, preserving its structure and activity. This is why subcutaneous administration is the default for peptides like BPC-157, TB-500, and most growth hormone secretagogues.
A few notable exceptions do exist:
- Collagen peptides have higher oral bioavailability because they are hydrolyzed into smaller fragments that survive digestion more readily.
- Oral formulations with protective matrices are being researched but are not yet standard practice for therapeutic peptide types.
- Intranasal peptides like Semax exploit the direct olfactory pathway to the brain, bypassing the gut entirely.
Understanding peptide types matters here because not all peptides share the same delivery constraints. But for the vast majority of bioactive peptides used in therapy and performance protocols, injection remains the evidence-backed route for reliable results.
Current evidence and clinical uncertainties in peptide dosing and administration
Getting comfortable with the injection process is only part of the picture. The harder reality is that many of the peptides generating buzz online don't yet have validated clinical dosing protocols. That's not a reason to panic, but it is a reason to be careful.
"Despite popularity, there is a critical lack of evidence supporting clinical use for many peptides, and dosing regimens remain unknown for many compounds."
This isn't an obscure footnote. It's the central challenge in peptide therapy today. You'll find no shortage of forums, influencers, and sellers willing to give you a "proven" dosing schedule, but most of those protocols are borrowed from anecdote, not clinical trial. The peptide efficacy gaps between animal studies and human applications are significant.
What this means in practice: dosing that works for one person may be excessive or insufficient for another, depending on body composition, health status, metabolism, and the specific peptide involved. Peptides used for injury recovery, metabolic optimization, or cognitive enhancement often operate at hormonal signaling levels, where small differences in dose can produce meaningfully different responses.
Rushing into stacking multiple peptides without physician oversight adds compounding unknowns. You're not just uncertain about one compound; you're stacking uncertainty on top of uncertainty. The stepwise peptide administration approach, working through one compound at a time with monitored results, is both safer and far more informative.
How to prepare and safely administer peptide injections: Essential steps
Safe peptide administration steps start well before the needle touches your skin. Preparation is where most errors happen, and errors here carry real contamination and potency risks.
Reconstitution process:
- Wash your hands thoroughly and prepare a clean, dry workspace.
- Wipe the rubber stopper of both the peptide vial and the bacteriostatic water vial with an alcohol swab. Let them air dry for 30 seconds.
- Draw the appropriate volume of bacteriostatic water into your syringe slowly.
- Insert the needle into the peptide vial at an angle and release the water gently down the inside wall of the vial. This minimizes foaming.
- Swirl the vial gently rather than shaking it. Shaking creates bubbles and can denature the peptide structure.
- Inspect the solution. It should be clear and free of particles. Do not use a cloudy or discolored solution.
Injection technique for subcutaneous use:
- Pinch a small fold of skin, typically on the abdomen or upper thigh.
- Insert the needle at a 45 to 90 degree angle depending on your needle length and tissue depth.
- Inject slowly and steadily, then withdraw the needle cleanly.
- Apply gentle pressure with a clean swab if needed. Do not rub.
Rotation matters more than most beginners expect. Injecting the same site repeatedly causes lipohypertrophy (a buildup of fibrous tissue under the skin) that reduces absorption rates and creates visible lumps. Map out at least four to six rotating sites and track your pattern.
Pro Tip: Draw up your dose using an insulin syringe in the 29 to 31 gauge range for significantly reduced injection discomfort compared to standard syringes. The small bore needle is well suited for subcutaneous administration and minimizes tissue trauma.

Peptide administration techniques extend to intramuscular peptide administration for some specific compounds. Intramuscular injections deliver into muscle tissue, typically the deltoid or vastus lateralis, and are used when faster or more localized absorption is needed. However, most peptide protocols use subcutaneous delivery unless otherwise specified by a prescribing provider. For a detailed walkthrough of selecting and preparing your protocol, a personalized peptide preparation guide can help you avoid the common setup mistakes. If any terminology in your protocol is unclear, reviewing peptide injection safety terms will save you time and confusion.
The importance of product quality and sterility in peptide administration
Where your peptide comes from is just as important as how you administer it. FDA-approved peptide drugs are backed by clinical evidence and strict manufacturing standards, while research-grade peptides often lack these assurances, affecting purity and safety. This distinction is not academic — it has direct consequences for what enters your body.
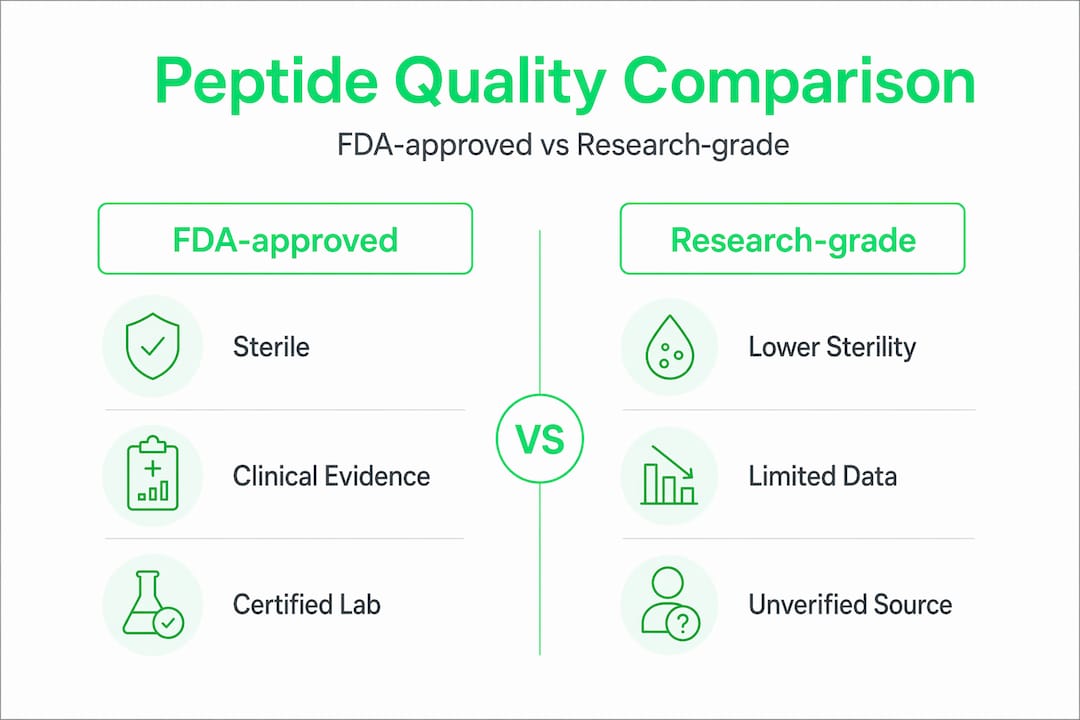
| Feature | FDA-approved peptides | Research-grade peptides |
|---|---|---|
| Clinical evidence | Required for approval | Often absent or limited |
| Manufacturing standards | Current Good Manufacturing Practice (cGMP) | Variable, often unverified |
| Sterility assurance | Terminal sterilization or validated aseptic processing | Not guaranteed |
| Purity testing | Mandatory third-party verification | Inconsistent |
| Legal status | Prescription or OTC as approved | Often sold for research only |
Terminal sterilization provides the highest sterility assurance and should be used unless technically unsuitable for the compound, while aseptic processing is a lesser alternative. The practical implication: peptides that cannot survive terminal sterilization must rely on aseptic processing, which requires the manufacturer to maintain an exceptionally controlled environment throughout production. Not all research-grade suppliers do.
Buying peptides from unverified online sources for self-directed synthetic peptide use introduces risks that no preparation technique can fully compensate for. A contaminated vial is still contaminated no matter how carefully you reconstitute it.
Pro Tip: Look for suppliers that provide independent, third-party certificates of analysis (COAs) with each batch. A legitimate COA shows purity percentages, amino acid sequence confirmation, and endotoxin testing results. If a vendor can't provide one, that tells you everything you need to know.
Best practices for optimizing personalized peptide administration
The benefits of peptide therapy depend entirely on how well the administration is executed, monitored, and adjusted over time. Getting this right is an active process, not a one-time setup.
- Start with one peptide at a time. Before stacking BPC-157 with TB-500, establish your individual response to each compound separately. This gives you a reliable baseline and makes it far easier to identify the source of any side effects.
- Use blood work before and during therapy. Common peptide side effects like altered cortisol, IGF-1 levels, or inflammatory markers won't announce themselves until labs do. Baseline panels give you something to compare against.
- Follow physician recommendations for dosing and frequency. Practitioners advise diagnosis-based indications and careful monitoring rather than self-directed stacking or frequent administration. This isn't bureaucratic advice — it's damage control.
- Maintain cold chain storage. Reconstituted peptides should be refrigerated at around 4°C and used within one month. Lyophilized (freeze-dried) powder stored correctly can last significantly longer.
- Track your biometric responses. Heart rate variability, sleep quality, recovery time, and body composition changes are all meaningful data points when monitoring peptide therapy outcomes.
- Stick to validated preparation and storage protocols. Improvising here, such as using regular bacteriostatic water substitutes or storing reconstituted peptides at room temperature, degrades your investment.
Following safe peptide therapy practices consistently is what separates users who see real, sustained results from those who run expensive protocols with nothing to show for it.
A fresh take on peptide administration: navigating uncertainty with informed caution
Here's the tension nobody in the peptide space talks about openly: the enthusiasm around these compounds is real, but the clinical infrastructure to support safe self-administration largely isn't there yet.
The community has moved faster than the science. That's not automatically a bad thing — early adopters always do. But it creates a specific problem: dosing protocols circulating online are often reverse-engineered from anecdote, and when something appears to work in a handful of cases, it gets treated as validated. It isn't.
Clinicians emphasize that peptide safety depends heavily on sourcing and administration under physician guidance with monitoring, due to the risks from unregulated products and unknown dosing. That's not a conservative dismissal of peptide therapy. That's a recognition that the margin for error is real, especially with compounds that influence hormone signaling, immune function, and tissue repair.
The nuanced position is this: understanding peptide administration means genuinely understanding the clinical evidence limitations, not just the injection technique. You can execute a perfect subcutaneous injection with properly reconstituted peptide from a sterile vial and still be following a dosing protocol built on nothing more solid than a fitness forum post.
The most effective users we see are the ones who treat this as a monitored experiment, not a fixed protocol. They work with prescribers, track biomarkers, respect the uncertainty, and adjust accordingly. That's not timid use of peptides. That's intelligent use.
Explore personalized peptide therapy support with Peptide AI
With a solid foundation in peptide administration, the next step is applying these principles with the right tools behind you.
Peptide AI is built specifically for this. The app catalogs 50+ peptides including BPC-157, TB-500, and Semax with peer-reviewed research backing every entry. You can build custom stacks, set precise dosing schedules, and track your biometric responses through integrations with Apple Health, Oura Ring, and Whoop. The AI Insights Chatbot gives you data-backed answers in real time, while the AI Body Scanner tracks your physical transformation over time. Whether you're just starting out or refining an existing protocol, Peptide AI puts research-grade intelligence in your hands so every administration decision is informed, not guesswork.
Frequently asked questions
Why are most peptides administered by injection instead of orally?
Most peptides degrade quickly in the digestive tract and have very low oral bioavailability of around 1 to 2%, so injection ensures they reach the bloodstream with their structure intact and active.
Are there established dosing guidelines for all peptides?
No. Dosing, frequency, and duration of treatment remain unknown for many peptides, which is why individualized physician supervision is essential rather than optional.
What risks come with using non-FDA-approved peptides?
Research-grade peptides often lack the sterility and purity standards of FDA-approved drugs, which increases the risk of contamination, inconsistent dosing, and adverse effects.
How should reconstituted peptides be stored?
Reconstituted peptides should be refrigerated at around 4°C and used within approximately one month to maintain potency and reduce contamination risk.
Can multiple peptides be mixed in one injection?
Some peptides can be combined into a single syringe safely if the solution remains clear and pressure is balanced, but always confirm with your provider before mixing compounds.