
BPC-157 is one of the most debated peptides in fitness and biohacking circles right now. Forums overflow with stories of torn tendons healing in weeks and chronic joint pain disappearing overnight, yet most of this enthusiasm is built on preclinical functional recovery data from animal models rather than large-scale human trials. For serious athletes and biohackers, that gap matters enormously. This guide cuts through the noise by examining exactly what the science shows, where the legitimate risks live, and how to manage a BPC-157 protocol intelligently if you choose to explore it.
Table of Contents
- What is BPC-157 and how does it work?
- The evidence: Animal studies vs. human trials
- Safety, legal status, and practical risks
- Protocol management: Expert tips for fitness and recovery
- The reality: Promising, but caution required
- Explore expert-guided peptide solutions
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Strong animal evidence | BPC-157 shows robust muscle and tendon repair in animal studies, but human data is still scarce. |
| Legal and quality risks | BPC-157 is not FDA-approved and banned in sports, with sourcing worries for research-grade peptides. |
| Protocol tips matter | Effective protocol management, including source quality and monitoring, maximizes safety for fitness recovery. |
| Angiogenesis caution | Its ability to boost blood supply can be risky in active cancer cases, so expert guidance is essential. |
What is BPC-157 and how does it work?
BPC-157, which stands for Body Protection Compound 157, is a synthetic 15-amino-acid peptide derived from a protein found in gastric juice. Researchers originally isolated it studying gastrointestinal healing, but its tissue-repair properties quickly attracted attention far beyond the gut. Today it sits among the most discussed peptide supplement types in the performance recovery space, and understanding its mechanism tells you a lot about both its promise and its limitations.
The peptide's two primary mechanisms are angiogenesis and fibroblast activation. Angiogenesis means it stimulates the formation of new blood vessels, which is critical for delivering oxygen and nutrients to damaged tissue. Fibroblast activation means it accelerates the proliferation of cells responsible for producing collagen, the structural protein in tendons, ligaments, and muscle fascia. Together, these actions create a tissue-repair environment that the body would otherwise generate far more slowly on its own.
"BPC-157 prioritizes angiogenesis and fibroblast activation as its core mechanisms for tendon and muscle repair, explaining its outsized effect in poorly vascularized tissue."
This is exactly why poorly vascularized tissues like tendons respond so dramatically in animal models. Tendons have notoriously low blood supply, which is why tendon injuries heal slowly and incompletely. A compound that can essentially build new blood vessels into the repair site is theoretically game-changing for that context. Understanding the broader peptide classifications helps you see where BPC-157 fits relative to growth factors, secretagogues, and other categories.
Key actions that make BPC-157 uniquely relevant for musculoskeletal repair:
- Promotes VEGF (vascular endothelial growth factor) upregulation for new vessel growth
- Activates fibroblasts to accelerate collagen synthesis in tendons and fascia
- Modulates nitric oxide pathways, improving local blood flow at injury sites
- Shows gastroprotective effects, protecting the gut lining under stress
- Demonstrates neuroprotective properties in certain animal models
The Croatian research teams at the University of Zagreb have driven most of the foundational preclinical work on BPC-157 over the past 30 years. Their studies cover everything from Achilles tendon transections to muscle crush injuries, and the results consistently favor BPC-157 as a repair accelerator. The critical caveat is that almost all of this work uses rodent models, which do not always translate cleanly to human physiology.
The evidence: Animal studies vs. human trials
Now that you know what BPC-157 is, let's compare the robust animal study data with what's actually been proven in people. The contrast is stark, and missing this distinction is where a lot of fitness enthusiasts go wrong.
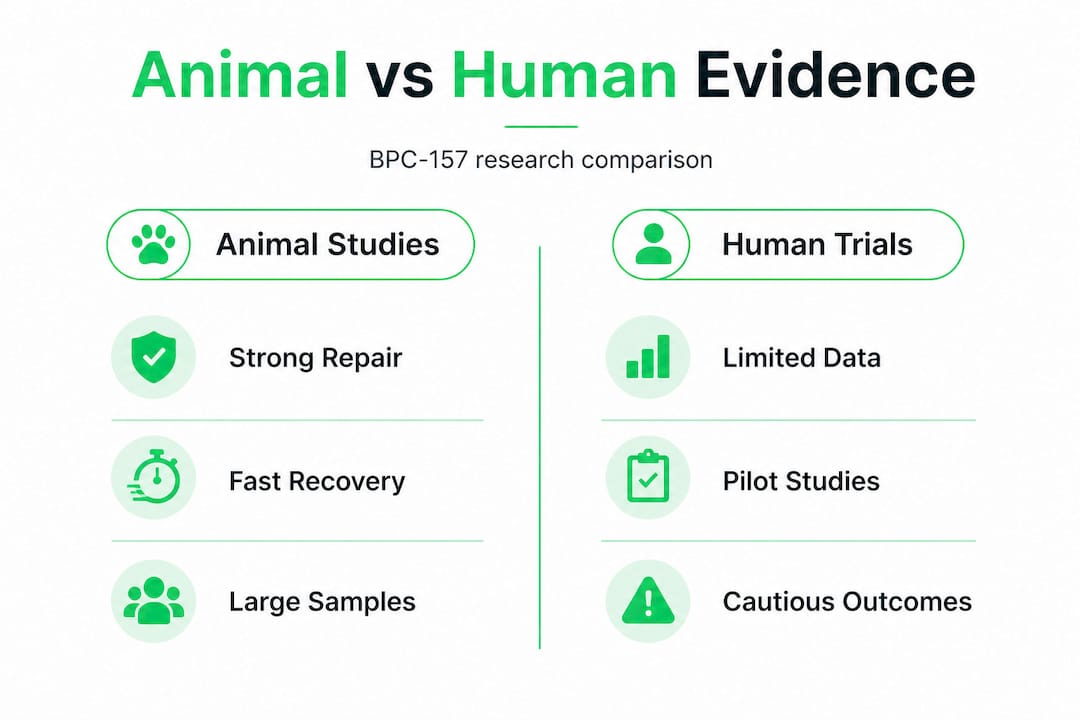
Animal studies paint an impressive picture. Rodent models show improved muscle fiber regeneration, reduced fibrosis after injury, and measurable functional recovery in tasks like grip strength and locomotion. Studies have demonstrated accelerated healing in Achilles tendon transection models, rotator cuff tear models, and even spinal cord injury models. These are not trivial findings. The consistency across injury types in multiple independent studies is genuinely compelling for researchers.

Human data tells a much more cautious story. The empirical human data consists primarily of small pilot studies and case series, not the large randomized controlled trials that establish clinical proof. Most human work focuses on knee pain and interstitial cystitis, not athletic soft tissue injuries. Even in these limited studies, results show roughly 80 to 90 percent symptom relief, but the sample sizes are too small to draw firm conclusions about mechanism, optimal dosing, or long-term safety.
| Factor | Animal studies | Human trials |
|---|---|---|
| Evidence volume | Hundreds of studies | Handful of pilots |
| Injury types studied | Tendon, muscle, gut, CNS | Knee pain, cystitis |
| Results | Strong functional recovery | 80-90% symptom relief |
| Study quality | Controlled, replicable | Small, uncontrolled |
| Conclusion | Mechanistically promising | Investigational only |
The numbered progression of evidence maturity in pharmacology typically looks like this:
- In vitro (cell culture) studies establish basic mechanism
- Animal models test safety and dose-response in living systems
- Phase I human trials establish basic safety in small groups
- Phase II trials test efficacy in targeted patient populations
- Phase III large RCTs establish proof for regulatory approval
BPC-157 is somewhere between steps 2 and 3 in most applications. That puts it firmly in the "promising but unproven" category for human use. For biohackers who track muscle growth science obsessively, this distinction is not semantic. It determines how much weight you should put on anecdotal reports versus measured self-experimentation.
There are also performance peptide examples with more robust human evidence that might pair better with BPC-157 in a stack, depending on your goals. The point is not to dismiss BPC-157 but to position it accurately within the evidence hierarchy.
Safety, legal status, and practical risks
While the evidence is intriguing, safety and legal status are crucial for anyone considering BPC-157 as part of a recovery protocol. Let's be clear and specific here because misinformation flows fast in this space.
What the safety data actually shows. No LD50 (lethal dose threshold) has been established in animal studies, meaning researchers have not found a toxic dose even at very high concentrations. No major adverse events have been reported in the limited human pilot studies conducted so far. That sounds reassuring, but remember the human study sample sizes are tiny. An adverse event profile built on a few dozen participants tells you very little about what happens across thousands of users over years of use.
Reported side effects in the real world tend to be mild and include:
- Nausea, particularly when taking oral or high-dose injectable forms
- Injection site redness, swelling, or discomfort
- Transient dizziness or fatigue reported anecdotally
- Potential interaction with anticoagulant medications due to nitric oxide effects
Legal and regulatory status is a major practical concern. BPC-157 is not FDA-approved for any indication. It was also added to the WADA banned substances list, meaning competitive athletes who test positive can face sanctions regardless of therapeutic intent. For recreational fitness enthusiasts, the legal risk is primarily around sourcing rather than competition bans, but the lack of regulatory oversight is a genuine safety issue.
| Risk factor | Detail | Impact level |
|---|---|---|
| FDA status | Not approved | High (legal/safety) |
| WADA status | Banned | High (competitive athletes) |
| Sourcing quality | Research chemicals vary widely | High (contamination risk) |
| Angiogenesis concern | Could stimulate tumor vascularity | High (cancer patients) |
| Short-term side effects | Mild nausea, injection reactions | Low to moderate |
The sourcing issue deserves special attention. Because BPC-157 is sold as a research chemical rather than a pharmaceutical product, quality control is inconsistent. Endotoxin contamination and underdosing are real problems in the research chemical market. Poor-quality peptide can cause inflammatory reactions or simply fail to work, and you would have no reliable way to know which problem you are dealing with. Understanding peptide safety and purity standards is non-negotiable before purchasing any research peptide.
One edge case that cannot be overstated: if you have a history of cancer or are currently in treatment, BPC-157's angiogenic properties present a real theoretical risk. Tumor growth depends heavily on vascularization. A compound that promotes new blood vessel growth could potentially support tumor vascularity. This is not a reason to panic if you are healthy, but it is a definitive reason to avoid BPC-157 if you have any active malignancy.
Pro Tip: Always request a certificate of analysis (COA) from any peptide supplier. A legitimate COA includes mass spectrometry data and endotoxin testing results. If a vendor won't provide one, walk away. Also look into performance and recovery peptides that have more established safety profiles if you're just starting your peptide journey.
Protocol management: Expert tips for fitness and recovery
Given the risks, what's the safest and most effective way to manage BPC-157 protocols for fitness and recovery? The answer comes down to precision, sourcing, and honest self-monitoring.
Localized injection beats systemic administration for musculoskeletal goals. When targeting a specific injury, local subcutaneous injection near the injury site delivers the peptide directly to the tissue that needs it. Systemic delivery via intravenous or distant subcutaneous injection distributes BPC-157 throughout the body, which may be appropriate for gut or systemic inflammatory conditions but introduces more widespread angiogenic activity than you need for a tendon repair. More targeted equals more efficient and potentially safer.
Typical dosing patterns in the literature and among clinicians experienced with peptide therapy range from 200 to 500 micrograms per day for injury protocols, often split into two administrations. Duration tends to run 4 to 8 weeks depending on injury severity. These are not FDA-approved guidelines, they are clinical observations from practitioners operating in the research or wellness space.
Practical protocol management checklist:
- Source from vendors who provide third-party COAs with mass spec data
- Reconstitute with bacteriostatic water and store correctly at 2 to 8 degrees Celsius after reconstitution
- Use localized injection for specific musculoskeletal injuries rather than systemic routes
- Log every dose, injection site, and any subjective recovery metrics in a structured tracking system
- Track sleep quality, training performance, and tissue pain scores to separate placebo from real effects
- Do not use if you have active cancer, consult a practitioner experienced in peptide therapy before starting
- Run baseline bloodwork so you have pre-protocol reference values
The BPC-157 usage workflow matters as much as the peptide itself. A disorganized protocol with inconsistent dosing and no tracking produces data that is impossible to interpret. If you cannot tell whether your tendon recovered because of BPC-157, improved training load management, or just time, you are flying blind on future protocol decisions.
Pro Tip: Pair BPC-157 with objective recovery metrics, not just how you "feel." Use a wearable to track HRV (heart rate variability) and sleep stage distribution during your protocol. Subjective pain scores combined with objective HRV trends give you a much stronger signal about whether recovery is actually accelerating.
The reality: Promising, but caution required
Here is the perspective that most articles on BPC-157 miss entirely: the fitness and biohacking community's enthusiasm for this peptide has outpaced the science by a significant margin, and that is a meaningful problem.
The preclinical data is genuinely interesting. We would be misrepresenting the research by calling it worthless. But the human data remains investigational, and there is a cognitive trap that affects even highly intelligent, data-driven athletes: we pattern-match from animal studies to our own bodies in ways that feel logical but are not supported by evidence. Rodents do not train five days a week, have 20 years of accumulated joint stress, or take multiple other supplements simultaneously. The translation problem is real.
The responsible approach for fitness enthusiasts and biohackers is not "avoid BPC-157 forever because the trials aren't done." It is "treat this as a self-experiment with rigorous tracking, not a proven intervention." That distinction changes everything about how you design a protocol, how you interpret your results, and how much confidence you place in the outcome.
What most articles also miss is the self-assessment dimension. A lot of people run a 6-week BPC-157 protocol, feel better, and attribute 100 percent of that improvement to the peptide. But they also slept more, reduced training volume during the protocol, added physical therapy, and possibly benefited from simple time-based healing. Without controlled self-experimentation and consistent logging, you cannot isolate the variable. The peptide therapy evidence framework matters precisely because it gives you a structure to evaluate these interventions honestly rather than confirming what you hoped would be true.
The bottom line: BPC-157 is one of the more mechanistically plausible peptides in the recovery space. The preclinical signal is consistent enough to take seriously. But "serious" means structured, cautious, well-tracked experimentation, not uncritical adoption based on forum posts. Until large RCTs exist, every person using BPC-157 is operating as an n-of-1 researcher. Treat yourself accordingly.
Explore expert-guided peptide solutions
If you are serious about integrating BPC-157 or any other peptide into a performance recovery protocol, the difference between results and frustration often comes down to tracking infrastructure and access to real data.
Peptide AI gives you everything you need to move from guesswork to evidence-driven protocol management. The app catalogs over 50 peptides including BPC-157, TB-500, and Semax, with precise dosing schedules built around peer-reviewed research. The AI Insights Chatbot delivers real-time, data-backed recommendations so you can ask protocol questions and get substantive answers. The AI Body Scanner tracks physical transformation over time, and seamless integration with Apple Health, Oura Ring, and Whoop means your biometric data works together with your peptide logs to give you a complete recovery picture. Serious optimization demands serious tools.
Frequently asked questions
Can BPC-157 speed up muscle recovery after injury?
Animal models show faster muscle healing and functional recovery, but human evidence remains limited to small pilots, and more research is needed before making clinical claims.
Is BPC-157 legal for athletes and fitness use?
BPC-157 is on the WADA banned list and is not FDA-approved, so U.S. competitive athletes should avoid it to remain compliant in competition settings.
What are the most common side effects of BPC-157?
Small human pilot studies report only mild effects like nausea and injection site reactions, with no major adverse events documented, though long-term data is lacking.
Should BPC-157 be avoided if you have cancer?
Yes, experts strongly recommend avoiding BPC-157 in active cancer because its angiogenic mechanism could theoretically promote tumor blood supply and accelerate growth.