
You put real effort into your peptide protocol, and the results still feel inconsistent. That frustration is more common than you think. Optimizing peptide results is not simply about picking the right compound and injecting it. It comes down to a chain of decisions: sourcing quality, dosing accuracy, administration timing, and ongoing biomarker monitoring. Get any one of those wrong, and even a well-researched protocol underdelivers. This guide breaks down exactly what it takes to build a protocol that actually works, from baseline preparation through troubleshooting stalled progress.
Table of Contents
- Key Takeaways
- Optimizing peptide results: what you need before you start
- How to build and adjust your dosing protocol
- Troubleshooting stalled progress and common mistakes
- What to realistically expect and when
- My honest take on what actually moves the needle
- Take your protocol further with Peptideai
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Start with bloodwork | Baseline panels give you a reference point to measure real change and catch safety issues early. |
| Source quality matters first | Verify purity through a Certificate of Analysis before any protocol begins. |
| Route of administration changes everything | Subcutaneous injection delivers 50-80% bioavailability versus under 2% for unmodified oral peptides. |
| Track biomarkers, not just feelings | Objective data is what separates a protocol you refine from one you guess at. |
| Timelines are longer than most expect | Structural benefits like body composition and anti-aging effects typically require 3 to 6 months of consistent use. |
Optimizing peptide results: what you need before you start
Most failed protocols are not execution failures. They are preparation failures. Before you calculate a single dose, three foundational pieces need to be in place.
Baseline health evaluation. Baseline bloodwork, including a CBC, CMP, fasting glucose, HbA1c, lipid panel, and IGF-1 where relevant, is the non-negotiable starting point. Without it, you have no reference point to evaluate whether your protocol is working or causing harm. For GH secretagogue protocols specifically, IGF-1 monitoring every 3 to 6 months is critical to avoid pushing levels into a supraphysiological range.
Legal and quality verification. The regulatory picture for peptides in the U.S. has tightened considerably. 19 widely used peptides were moved to Category 2 status as of 2023 to 2024, prohibiting their compounding by licensed pharmacies. That does not stop the gray market, which means sourcing risk is real. Any peptide you use should come with a third-party Certificate of Analysis confirming purity above 98%, correct identity, and acceptable endotoxin levels. Unverified "research use only" peptides carry genuine risks of mislabeling, impurities, and contamination.
Route of administration. This is probably the most underestimated variable in understanding peptide protocols. Subcutaneous injections achieve 50 to 80% bioavailability while unmodified oral peptides typically deliver less than 2% due to proteolytic breakdown in the gut. Intranasal routes like Semax fall somewhere in between and work specifically because the peptide bypasses first-pass metabolism. Your choice of administration route determines the effective dose before you calculate anything else.
Here is a quick-reference comparison of the three most common routes:
| Route | Bioavailability | Common peptides | Key consideration |
|---|---|---|---|
| Subcutaneous injection | 50-80% | BPC-157, TB-500, CJC-1295 | Highest bioavailability, most consistent |
| Intranasal | 10-40% | Semax, Selank | Convenient, peptide-specific effectiveness |
| Oral (unmodified) | Under 2% | Most peptides | Proteolysis destroys most compounds |
Pro Tip: Set clear, measurable goals before you start. "More energy" is not trackable. "Improve HRV by 10% over 8 weeks" is. Goal specificity determines what biomarkers you monitor and how you know when to adjust.
How to build and adjust your dosing protocol
This is where the real work of maximizing peptide efficacy happens, and where most self-directed users make costly mistakes.
-
Calculate net peptide content, not gross weight. This is the single most common dosing error. Peptide powders contain counterions, most often trifluoroacetic acid (TFA), that make up a portion of the gross weight. If you dose by gross weight alone, you are almost certainly under-dosing. Net peptide content adjustment using amino acid count and TFA counterion estimates drastically improves dosing accuracy. Your Certificate of Analysis should list net peptide content. If it does not, contact the supplier before proceeding.
-
Reconstitute carefully. Add bacteriostatic water by directing it gently down the side of the vial. Never inject water directly onto the peptide cake. Swirl, do not shake. Mechanical agitation degrades peptides, particularly at lower concentrations. At very low concentrations, adding 0.1% BSA (bovine serum albumin) prevents adsorption losses to the vial walls.
-
Start lower and titrate up. This is the principle that separates experienced users from impatient ones. Starting at 50% of your target dose for the first one to two weeks lets you identify sensitivity and side effects before committing to full dosing. Skipping titration is the fastest way to attribute a bad reaction to the wrong variable.
-
Sequence your stack deliberately. If you run multiple peptides, timing matters. BPC-157 and TB-500 work synergistically for tissue repair and are commonly run together. Growth hormone secretagogues like CJC-1295 and Ipamorelin are most effective taken fasted, typically before bed, to align with natural GH pulse timing. Stacking without regard to timing means you may be working against your own physiology.
-
Cycle with intention. Personalized, data-driven protocols with ongoing biomarker monitoring outperform generic or indefinitely run stacks. A standard approach is 8 to 12 weeks on, followed by a 4-week break, with biomarker reassessment at the end of each cycle. This gives your body time to respond, gives you data to evaluate, and reduces receptor desensitization risk.
-
Store peptides correctly. Lyophilized (freeze-dried) peptides are stable at room temperature for short periods but should be refrigerated. Once reconstituted, store at 2 to 8°C and use within 30 days. Repeated freeze-thaw cycles degrade the compound. Label each vial with the reconstitution date.
Pro Tip: Keep a daily protocol log noting dose, time, injection site, and any subjective response. You cannot optimize what you do not track. Even a basic spreadsheet outperforms memory when you are troubleshooting six weeks into a cycle.
Troubleshooting stalled progress and common mistakes
Even a well-designed protocol can stop delivering. Here is how to diagnose what is actually going wrong.
-
Poor peptide quality. If you notice unusual color, particulate matter in solution, or smell anything off during reconstitution, discard the batch. Visible degradation or contamination is not a subtle signal. More commonly, quality issues show up as a complete absence of expected effects. If two weeks of a compound that reliably causes a response in published data produces nothing, question the source before questioning the protocol.
-
Dosing errors from skipping net peptide correction. If you calculated your dose using gross weight, recalculate. You may be running at 70% of your intended dose. This is especially relevant for peptides with high TFA content.
-
Ignoring adverse signals. Water retention, joint pain, tingling, and elevated fasting glucose are signals to reduce or pause a protocol, not push through. Comprehensive bloodwork is the most practical tool you have to evaluate whether something is moving in the wrong direction.
-
Regulatory and sourcing pitfalls. Buying the cheapest available product from an unverified vendor is a false economy. Third-party testing confirming purity above 98%, correct identity, and endotoxin levels is the minimum bar. The FDA's current peptide regulations reflect a precautionary stance that has created a gap between what research supports and what is commercially available through legitimate channels. Understanding that gap protects you.
-
Stalled progress mid-cycle. If your biomarkers and subjective response plateau, consider adjusting the dose by 10 to 15% in either direction before abandoning the protocol. Some peptides exhibit bell-curve dose-response relationships, meaning more is not always better. A structured peptide effectiveness approach acknowledges that protocol recalibration, not protocol abandonment, is the right response to stalled results.
"Peptide therapy optimization is not a one-time calibration. It is an ongoing process of data collection, interpretation, and adjustment. The practitioners seeing the best results treat each cycle as an experiment with defined endpoints."
What to realistically expect and when
One of the biggest mistakes people make when first building a protocol is expecting linear, rapid results. Peptide therapy follows a staged timeline, and understanding that timeline is part of how to optimize peptide protocols effectively.
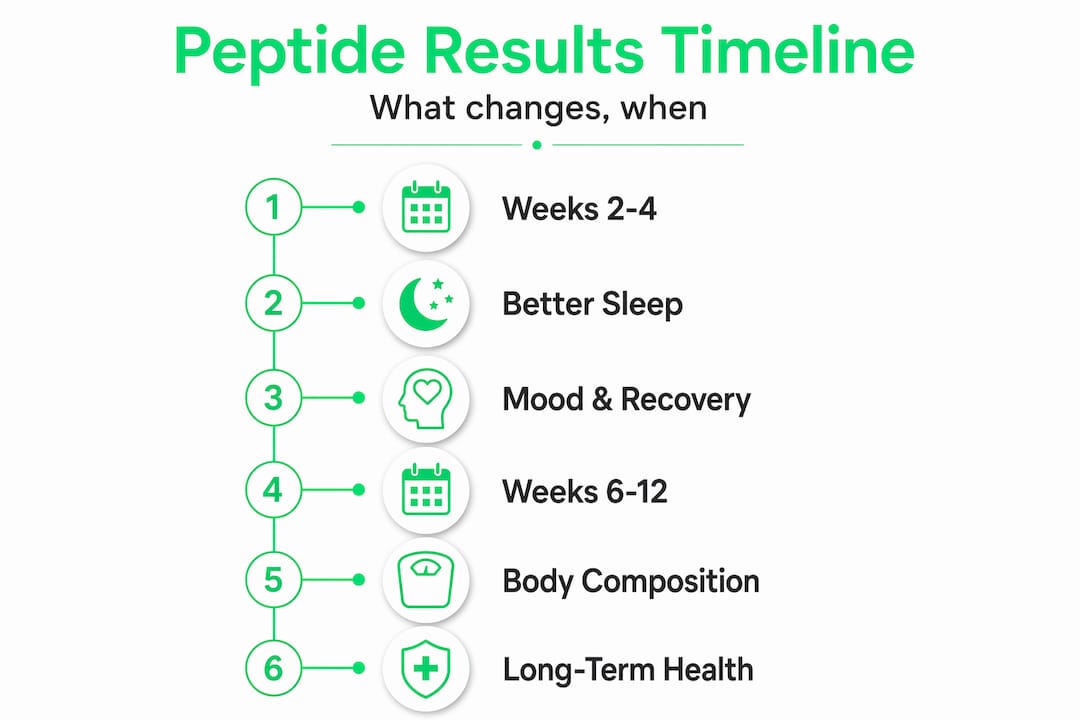
| Outcome | Typical timeline | Key driver |
|---|---|---|
| Improved sleep, mood, recovery | 2 to 4 weeks | Neurological and hormonal priming |
| Fat loss, libido, energy changes | 6 to 12 weeks | Metabolic and endocrine adaptation |
| Visible body composition changes | 3 to 6 months | Structural remodeling |
| Anti-aging and tissue repair effects | 3 to 6 months | Cellular regeneration processes |
The pattern here is clear: early wins are neurological and systemic, structural changes come later. If you are running BPC-157 for gut healing or joint repair, subjective improvement in discomfort often appears within weeks, but tissue-level regeneration continues for months. Setting expectations this way prevents people from abandoning a working protocol too early.
Integrating peptide therapy into a broader health strategy, including optimized nutrition, consistent resistance training, and quality sleep, enhances outcomes significantly. No peptide compensates for chronic sleep deprivation or a highly inflammatory diet. The peptide protocol is the modifier; your lifestyle is the foundation.

My honest take on what actually moves the needle
I have seen people run $600 worth of peptides and get nothing because they never verified their source had a real CoA, they dosed by gross weight without adjusting for net content, and they had no baseline labs to tell them whether anything was actually changing. That is not a peptide failure. That is a preparation failure.
What I have found to be true consistently: the individuals who get real, measurable results approach each cycle the way a researcher would approach an experiment. They define their endpoint before they start. They test before and after. They document every variable they can control. When something does not work, they change one variable at a time rather than scrapping everything.
The legal and sourcing challenges are real, and I will not pretend otherwise. But navigating them is not impossible. It requires doing the verification work upfront instead of trusting marketing copy. A third-party CoA is not optional, it is the price of entry for anyone serious about peptide cycle optimization.
What I have also learned is that individualized peptide protocols beat generic stacks every time. Your baseline labs, your goals, your lifestyle context, and your response data are all inputs that shape what your protocol should look like at month three versus month one. Anyone selling you a one-size protocol is selling you something that works for an average person in a study, not for you specifically.
— Sam
Take your protocol further with Peptideai
If you are serious about getting the most from your peptide therapy, the difference between guessing and knowing comes down to the quality of your tracking and the intelligence behind your adjustments.
Peptideai is built for exactly this. The app catalogs 50+ peptides including BPC-157, TB-500, Semax, and CJC-1295, with precise dosing schedules and net peptide content calculations built in. You can integrate data from Apple Health, Oura Ring, and Whoop to track how your biomarkers respond across a full cycle. The AI Insights Chatbot gives you real-time, research-backed recommendations when you need to adjust. And the AI Body Scanner creates a visual record of your physical transformation over time. If you are ready to run a protocol backed by data instead of guesswork, explore Peptideai and see what a research-grade approach actually looks like in practice.
FAQ
What is peptide optimization?
Peptide optimization is the process of systematically adjusting dosing, timing, administration route, and monitoring to get the maximum therapeutic effect from a peptide protocol while minimizing safety risks.
How long before you see results from peptide therapy?
Initial improvements in sleep, mood, and recovery typically appear within 2 to 4 weeks, while structural changes like body composition and visible tissue repair require 3 to 6 months of consistent use.
Why does route of administration matter so much?
Subcutaneous injection delivers 50 to 80% bioavailability, while unmodified oral peptides typically deliver under 2%. Choosing the wrong route can make an otherwise correct dose functionally ineffective.
How do I know if my peptides are high quality?
Request a Certificate of Analysis from an independent third-party lab confirming purity above 98%, correct identity, and acceptable endotoxin levels. Do not rely on vendor claims alone.
When should I adjust my peptide protocol?
Adjust when your biomarker data plateaus, when adverse signals appear, or when you complete a full cycle. Change one variable at a time so you can accurately identify what is driving any change in response.