If you've been researching growth hormone peptides, you've likely hit a wall of contradictory claims, confusing terminology, and hype that outpaces the actual science. What is growth hormone peptide, exactly, and how does it differ from simply injecting synthetic HGH? The distinction matters enormously, both for your results and your safety. Growth hormone peptides are not a shortcut or a replacement for the hormone itself. They are signaling compounds that tell your body to produce more of its own growth hormone, working with your physiology rather than around it. This guide breaks down the mechanisms, the evidence, and the protocols worth following.
Table of Contents
- What are growth hormone peptides and how do they work?
- Types of growth hormone peptides: GHRPs, GHRH analogs, and secretagogues
- Growth hormone peptides for muscle recovery and performance: evidence and effects
- Using growth hormone peptides safely: protocols, timing, and risks
- Why a balanced, informed approach to growth hormone peptides matters
- Get started with growth hormone peptides safely at Peptide AI
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Growth hormone peptides stimulate natural GH | These peptides work by triggering your pituitary gland to release your own growth hormone rather than replacing it directly. |
| Different peptide types vary in action | GHRH analogs and GHRPs have distinct mechanisms and benefits, with tesamorelin being the only FDA-approved peptide for a specific condition. |
| Peptides support muscle recovery and aerobic capacity | Scientific studies show GH peptides can increase muscle volume and aerobic capacity, aiding fitness recovery. |
| Safe use requires timing and cycling | Stacking GHRH analogs with GHRPs and dosing at night aligns with natural pulses, while long-term use should be cycled to prevent desensitization. |
| Monitor and personalize protocols | Tracking IGF-1 levels and adjusting doses helps maximize benefits and minimize risks during peptide use. |
What are growth hormone peptides and how do they work?
Growth hormone peptides fall into a category called GHRPs, or growth hormone-releasing peptides. These are small synthetic peptides that enhance GH release from your pituitary gland rather than delivering growth hormone externally. The first active synthetic GHRP, GHRP-6, was developed in 1984. That timeline matters because it means there are now decades of research behind these compounds, not just a few years of biohacker experimentation.
To understand why this approach is different from synthetic HGH, you need to know what natural growth hormone actually is. Human growth hormone (hGH) is a 191-amino acid hormone secreted by the pituitary gland. It drives growth, regulates metabolism, supports tissue repair, and influences body composition. After adolescence, natural GH production declines steadily. Somatropin, the synthetic version of hGH, was FDA-approved in 1985 as a direct replacement for patients with clinically diagnosed GH deficiency.
Here is where most people get confused. Somatropin replaces the hormone. GHRPs stimulate your pituitary to release the hormone it is already capable of producing. That difference has real implications for how your body regulates GH levels and how much risk you take on.
Key distinctions at a glance:
- GHRPs trigger endogenous (your own) GH secretion via pituitary stimulation
- Synthetic hGH bypasses the pituitary entirely and delivers hormone directly
- GHRPs preserve natural feedback loops; synthetic GH can override them
- Peptides aid muscle growth through pathways that also support recovery and repair
- GHRP action is dose-dependent and tied to natural GH pulse timing
Understanding this foundation changes how you approach dosing, timing, and stacking. You are not flooding your system. You are nudging it.
Types of growth hormone peptides: GHRPs, GHRH analogs, and secretagogues
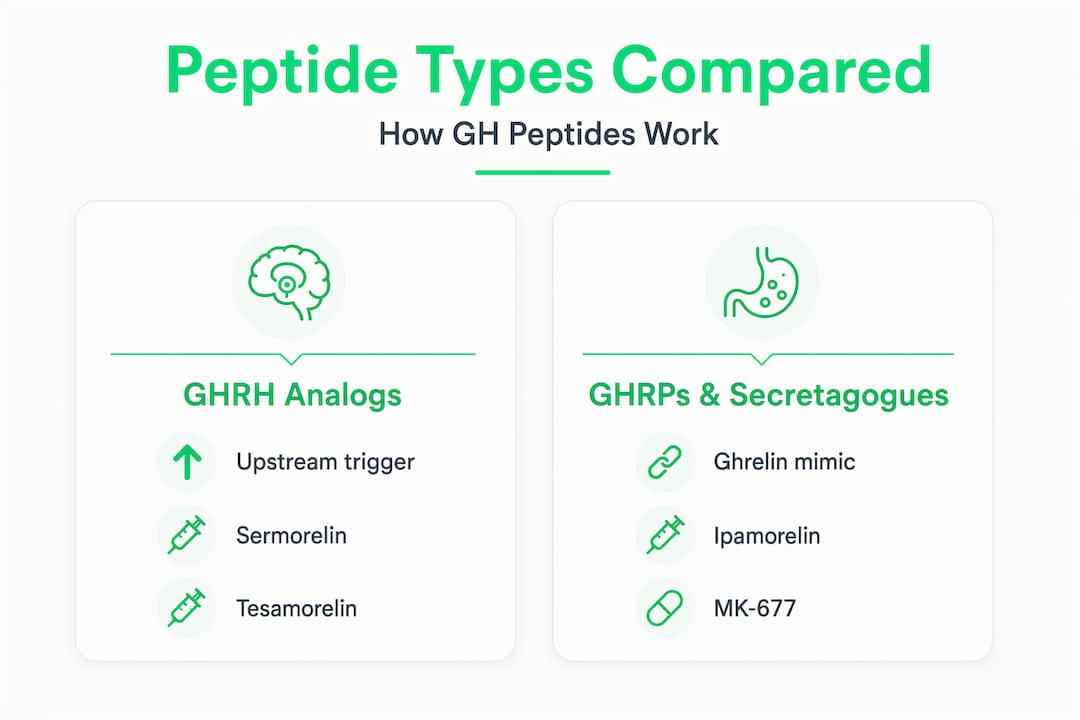
The term "growth hormone peptide" covers several distinct compound classes, and treating them as interchangeable is a common mistake. Growth hormone secretagogues stimulate the pituitary to release GH through three main categories: GHRH analogs, GHRPs (ghrelin mimetics), and oral secretagogues like MK-677.
GHRH analogs such as sermorelin and tesamorelin mimic the body's own growth hormone-releasing hormone. They work upstream, telling the pituitary to produce a GH pulse. Tesamorelin is FDA-approved but only for HIV-associated lipodystrophy, not for general adult GH deficiency or performance use. No other GHS peptides have FDA approval for adult GH deficiency. That is a critical regulatory reality every fitness user should understand.

GHRPs like ipamorelin and GHRP-2 mimic ghrelin and bind to the GHS-R1a receptor in the pituitary and hypothalamus. Ipamorelin is particularly valued because it selectively stimulates GH release with minimal impact on cortisol or prolactin, making it one of the cleaner options in this class.
MK-677 (ibutamoren) is not technically a peptide but is an oral non-peptide secretagogue. It also acts on GHS-R1a and produces sustained GH elevation, though its oral bioavailability comes with different risk and dosing considerations.
| Peptide | Type | Mechanism | FDA Status |
|---|---|---|---|
| Sermorelin | GHRH analog | Stimulates pituitary GHRH receptors | Not approved for general use |
| Tesamorelin | GHRH analog | Stimulates pituitary GHRH receptors | Approved for HIV lipodystrophy only |
| Ipamorelin | GHRP/ghrelin mimetic | Binds GHS-R1a, selective GH release | Not FDA-approved |
| GHRP-2 | GHRP/ghrelin mimetic | Binds GHS-R1a, less selective | Not FDA-approved |
| MK-677 | Non-peptide secretagogue | Oral GHS-R1a agonist | Not FDA-approved |
| Somatropin | Recombinant hGH | Direct hormone replacement | FDA-approved for GH deficiency |
Knowing which peptide supplement types you are dealing with determines not just your protocol but your risk profile. GHRH analogs and GHRPs are frequently stacked together because they work on different receptors and produce synergistic GH pulses.
Pro Tip: Combining a GHRH analog (like sermorelin) with a GHRP (like ipamorelin) can amplify GH release more than either compound alone, because they act on complementary pathways. This is the foundation of most evidence-informed GH peptide stacking protocols.
Growth hormone peptides for muscle recovery and performance: evidence and effects
This is where fitness enthusiasts tend to get either overly skeptical or dangerously optimistic. The evidence is real but nuanced. Let's be specific about what the data actually shows.
Clinical research on GH replacement in deficient adults found that GH substitution increases aerobic exercise capacity by 8.9% and VO2 max by 0.17 L/min. Muscle volume improved by 7.1%. Muscle strength gains, however, were modest at 3.2% and did not reach statistical significance. In other words, you will likely see real changes in body composition and aerobic capacity, but expecting dramatic strength increases purely from GH peptide use is an overclaim.
Beyond body composition, GHRP and GHRH peptides are recognized for speeding tissue repair and stimulating HGH secretion in ways that influence growth, metabolism, and recovery. These are the mechanisms that make them genuinely interesting for peptides for muscle recovery after high-volume training.
Documented growth hormone peptide benefits for fitness:
- Improved aerobic capacity: Measurable increases in VO2 max and exercise endurance
- Enhanced muscle volume: Statistically significant gains in lean tissue over time
- Accelerated tissue repair: GH promotes collagen synthesis and cellular regeneration
- Fat metabolism: Increased lipolysis, supporting body recomposition
- Sleep quality improvement: GH peaks during deep sleep; peptides that support nocturnal GH pulses often improve sleep architecture
"Some peptide benefits for acute injury recovery remain anecdotal, but the mechanisms supporting their use in workout recovery and muscle growth are grounded in established HGH physiology."
Tracking progress objectively matters. IGF-1 (insulin-like growth factor 1) is the downstream marker that best reflects sustained GH activity. Monthly IGF-1 testing gives you a concrete signal of whether your protocol is working and whether you are staying within a safe physiological range.
| Outcome | Effect size | Evidence quality |
|---|---|---|
| Aerobic capacity (VO2 max) | +8.9% | Clinical trial |
| Muscle volume | +7.1% | Clinical trial |
| Muscle strength | +3.2% (NS) | Clinical trial |
| Tissue repair rate | Positive signal | Mechanistic/anecdotal |
| Fat mass reduction | Measurable | Clinical/observational |
Pro Tip: Track your IGF-1 before starting any GH peptide protocol, at 6 weeks, and at 3 months. This gives you a baseline, a trend line, and a safety ceiling all at once.
Using growth hormone peptides safely: protocols, timing, and risks
How you use these compounds matters as much as which ones you choose. Getting the protocol wrong does not just reduce your results. It can dysregulate your hormonal axis in ways that take months to recover from.
Core principles for safe GH peptide use:
- Stack GHRH and GHRP compounds together for synergistic GH pulses that better mimic natural pituitary secretion patterns
- Cycle your use. Continuous peptide use beyond 3 to 6 months risks pituitary desensitization. Plan breaks into your protocol from the start
- Dose conservatively and titrate up. Starting at the low end of the therapeutic range and adjusting based on IGF-1 response is more intelligent than front-loading high doses
- Time your doses strategically. Ipamorelin at bedtime aligns with your body's natural nocturnal GH peak, amplifying a pulse that is already occurring rather than creating an artificial one at the wrong time
- Monitor for growth hormone peptide side effects including water retention, joint discomfort, tingling or numbness in extremities, and elevated fasting glucose. These are your early warning signals, not acceptable background noise
- Get bloodwork done. IGF-1, fasting insulin, glucose, and a thyroid panel give you the data you need to make informed adjustments
Understanding safe peptide protocols also means understanding what you should not do. Running high-dose GHRP-2 continuously, skipping bloodwork, or stacking multiple secretagogues without understanding their combined receptor activity are all patterns that turn manageable compounds into unnecessary risks.
The question "are growth hormone peptides safe?" does not have a universal answer. Safety depends entirely on compound selection, dosing, cycle length, individual health status, and monitoring rigor. For a healthy adult with no underlying GH-axis dysfunction who follows a calibrated protocol and gets regular bloodwork, the risk profile is reasonable. For someone who doses by feel and never checks IGF-1, the risk profile is entirely different.
Why a balanced, informed approach to growth hormone peptides matters
Here is an uncomfortable truth most content on this topic avoids. The appeal of synthetic GH has always been simplicity. One injection, a known dose, predictable pharmacokinetics. But synthetic GH injections risk supraphysiologic hormone levels because they bypass the natural pulsatility your pituitary is designed to maintain. That regulatory mechanism exists for good reasons. Your feedback loops govern not just GH but IGF-1, insulin sensitivity, and downstream tissue responses. Override them consistently and you introduce risks that go well beyond water retention.
Growth hormone peptides are more sophisticated, not less. They work with your pituitary's existing architecture. That is their real advantage, and it is also why they require more understanding to use well. A compound that respects your physiology still demands that you understand that physiology.
The biohacker community has sometimes framed GH peptides as a smarter alternative to exogenous GH, and in mechanistic terms, that framing holds up. But "smarter" does not mean consequence-free. It means the risk and reward profile is different, not absent. The users who get the most out of peptide research and safety are not the ones chasing the fastest gains. They are the ones who treat IGF-1 data like training data, adjust protocols based on what their body reports, and think in months rather than weeks.
Long-term peptide optimization is not a sprint. The evidence supports meaningful improvements in recovery, body composition, and aerobic capacity when these compounds are used with discipline and measured expectations. The people who get burned are typically the ones who skip the monitoring, ignore the cycling protocols, or dose based on anecdotal forum advice rather than their own biomarker data.
Get started with growth hormone peptides safely at Peptide AI
If you are ready to move from theory to a structured, data-informed protocol, you need more than information. You need a system that tracks your stack, your dosing schedule, and your biometric response over time.
Peptide AI was built specifically for this. The app catalogs over 50 peptides including ipamorelin, sermorelin, BPC-157, and TB-500, allowing you to build custom stacks with precise dosing schedules backed by peer-reviewed research. The AI Insights Chatbot delivers real-time protocol recommendations based on your goals and biomarkers. The AI Body Scanner tracks physical transformation over time, and native integration with Apple Health, Oura Ring, and Whoop means your wearable data feeds directly into your peptide protocol. If you are serious about applying this science safely, the Peptide AI platform puts research-grade intelligence in your pocket.
Frequently asked questions
What is the difference between growth hormone peptides and synthetic human growth hormone?
Growth hormone peptides stimulate your body's natural GH release through pituitary signaling, while synthetic hGH replaces the hormone directly from an external source. Peptides preserve natural feedback loops; synthetic GH bypasses them entirely.
Are any growth hormone peptides FDA-approved for general adult use?
No. Only tesamorelin holds FDA approval, and that is specifically for HIV-associated lipodystrophy. No GHS peptides are approved for adult GH deficiency or general performance use as of 2026.
How do growth hormone peptides help with muscle recovery?
They stimulate endogenous HGH secretion, which drives tissue repair, collagen synthesis, and metabolic support. Peptides speed tissue repair and support the hormonal environment your muscles need to recover between training sessions.
What are the risks of using growth hormone peptides incorrectly?
Continuous use beyond 3 to 6 months can cause pituitary desensitization, and overdosing risks supraphysiologic IGF-1 levels with downstream metabolic effects. Cycling and monitoring are not optional extras. They are what separates a productive protocol from a problematic one.